Basic Anatomy Review
You have these parts for life, why not get to know them? First, structure creates function. Knowing how things are built together can tell you how they work together. Leonardo Da Vinci was a brilliant man, as he discovered how the human form renders its function. As an artist, he did most of his work with the external muscle and skeletal form, but the same concept surfaces here. You need to know what your parts look like and then it is easier to understand how everything works.
The female system is comprised of the ovaries, tubes, uterus, cervix, vagina, and bladder. I will also include information about the rectum. Note the physical relationship between the organs from the front views and side views. (Figure 1-front view and Figure 2-side view) Let’s start at the “bottom”. The opening of the vagina is called the vestibule while the length of the vagina is called the vault. The vagina is essentially a cylinder-like shape and at the top it is connected to the cervix. The vagina is made of a muscular wall and blood vessels. The lining, or mucosa, faces the inside. The muscle is what allows it to maintain its shape and to help support the bladder above it and keep the rectum back. It also can stretch wider for childbirth.
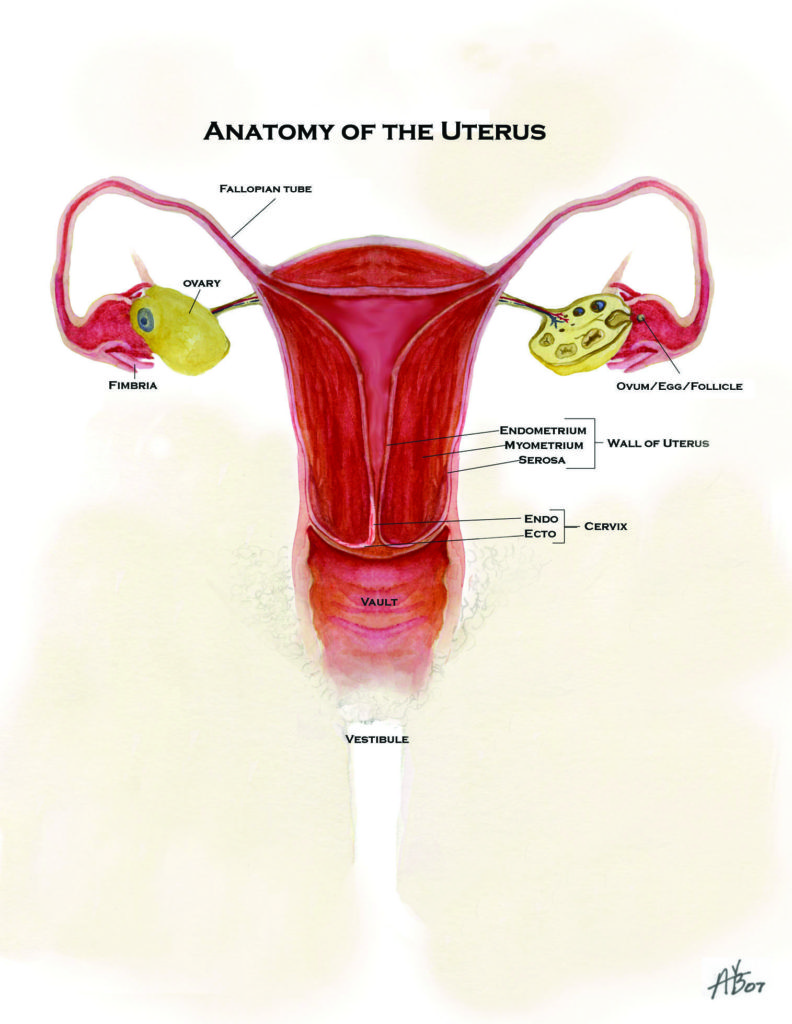
The cervix is at the top of the vagina and is contiguous with the uterus. (Figure 3) Visually trace the uterus from its top most area and then downward where it becomes the cervix. The cervix has an inside and an outside. The type of cells and function of the cells changes as the transition from the cervix to uterus happens. The outside of the cervix (where it contacts the vagina) is the ectocervix. The part of the cervix that is at the bottom of the uterus is the endocervix. Pap smears are done by brushing the outside and the inside for samples. A whole chapter is dedicated to that can of worms topic.
The tubes are small with trumpet shaped openings near the ovaries. The width of them is similar to a pencil. Tubes have microscopic hairs inside them to help sweep bacteria out and sweep sperm, eggs, and embryos (all the good stuff) along. They are very fragile. Ovaries are a complex surprise. They have millions of eggs in all stages of development and a stroma, or tissue, where hormone interactions occur. The eggs “rest” in the stroma. Picture if you will eggs sitting in a bird nest, which the concept and imagery are strikingly similar. Did you know that we are born with all of the eggs we will ever have? Men just keep making their swimmers, but we get the finite pool of eggs. I’ll get to that later.
The uterus is lodged in between the cervix and tubes. Going from inside to outside, several layers are stacked. The inside lining, or endometrium, is closest to the inside cavity and it “sheds” off with menstruation. Muscle layers lie beneath the lining and they make the wall of the uterus. The muscle wall of the uterus is not like the muscles we use to move our limbs. They are smooth muscle and respond to hormones. Position of the uterus varies between women, with the most common being slightly tilted forward, like in Figure 2. The majority of women have some tilt. The old phrase “you have a tilted uterus” is meant to refer to the women where there is a slight backwards tilt. Tilt does not mean anything about fertility, pap smears, periods, etc. It is not abnormal, only a variation of possibilities. A rare percentage of women can have a “double” uterus. It is weird but true. I have delivered ladies like this before. The first time was while I was a resident and my attending kept saying, “You got yourself a uterus like a dog.” I thought he was just being crass until I went home and looked it up on the internet. True.
Bladders are unique, and can be troublesome for women. Look very carefully at how it is positioned in relation to the vagina and uterus in Figure 2. Simply, it is for storage of urine and it is made of stretchable muscle with a thin lining on the inside. It is supported by the strong muscle wall of the vagina which is underneath it. The urethra is the tube that urine travels down to get out. It has got to cross your mind: how does urine not just constantly leak out if it is like an upside down bottle with no plug? There is a ring of muscle at the base of the bladder before the urethra starts. It is called the sphincter. We have control over this sphincter, like controlling a garage door opener. Our body tells it to remain shut in its natural state. That is why we do not walk around with urine coming out like a leaky faucet. Normally, the sphincter remains tightened or closed while the muscle of the bladder is told to relax. This allows the bladder to store urine without leaking out. When the bladder gets to a certain volume, nerves are triggered that tell our brain “you need to urinate”. We then go to the toilet and control the opening of the sphincter. The bladder muscle then contracts, which pushes out the urine.
On the back side of the vagina is the rectum mainly for evacuation of the bowels. The rectum is also held back from falling into the vagina by the strong muscular wall of the vagina. Another sphincter, or ring of muscle, is at the bottom edge of the rectum. Like the bladder sphincter, it normally is closed which would make sense so stool does not constantly fall out. Thank heavens for sphincters, or we would all be wearing diapers. The same mechanism that I described in the bladder happens when the rectum fills with stool. Nerves send a message to the brain to tell you about the bowel movement, and then the sphincter is voluntarily relaxed, which opens it. Gosh, thank heaven for sphincters.
Do you know your vagina? Take a look at it. Don’t be afraid, it will not bite you. I promise. I have a hand mirror for patients to use in every exam room so women can see what I see instead of trying to describe in words where I see something or where they think they see something. The visual impact holds in the memory better that saying, “It is a little to the left and downwards but in the middle of that space you have between your vaginal opening and rectum.” Wouldn’t you rather have a mirror and be shown?
Lie down on the bed or stand with one leg on a chair and take a mirror and look. (Figure 4) Find your urethra, pubic bone, perineum (space between vagina and rectum). Be familiar with your labia major and minor. Check it out, it is good for you. The female labia are very sensitive to touch and stimulation. Size does not matter and everyone’s labia look different. The labia minor can be long, protrude, dangle, and be smooth, darker or lighter in color. Just like sweat glands elsewhere in the body, the labia and vagina area have these also, which contributes to lubrication for sex.
The clitoris is the female counterpart to the penis, funny as that may seem. After sex or when aroused, it can be enlarged and swollen, sound familiar? So from top to bottom, you will see: clitoris, urethra, vaginal opening, and then rectal opening.
You need to know where things are and how they work together. Some things can go in there and other things do not belong in there at all, like kielbasas. The particular way the female pelvic organs are placed and work together in space and form is fascinating. Structure creates function. Your body is what makes you a woman. Know it. Love it. Protect it and treat it well. Next, venture forward to unearth the mystery of the menstrual cycle. Keep going through the chapters and you will find more than you ever thought you could know, want to know, or even things you didn’t know that you should know. It will all become clear.
Your Girlfriend GynecologistTM
Your Girlfriend GynecologistTM
Your Girlfriend GynecologistTM
Your Girlfriend GynecologistTM
Allyn G. Schaub M.D.
Your Girlfriend GynecologistTM